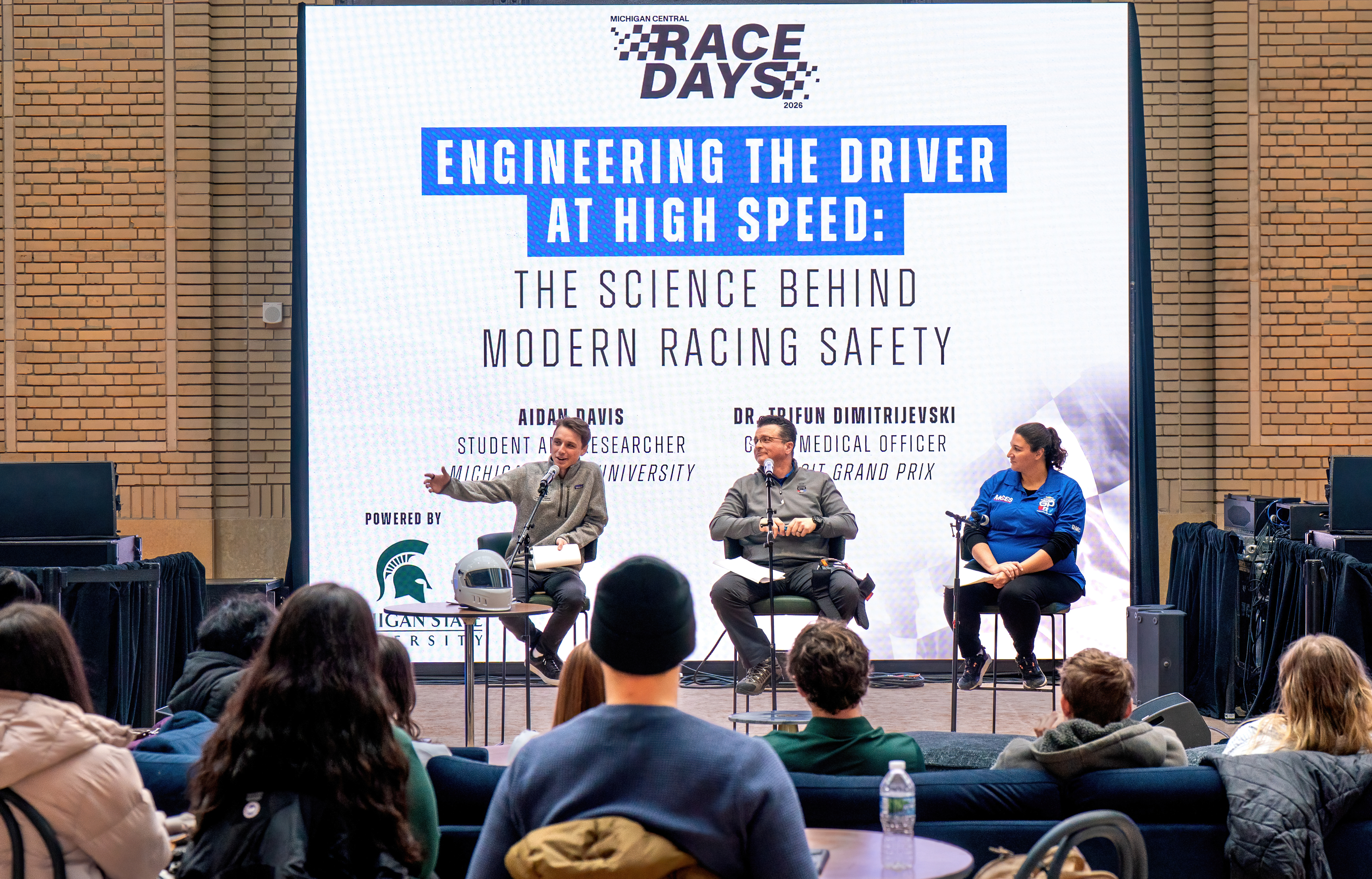
Second-year Michigan State University College of Osteopathic Medicine student Aidan Davis kicked off a presentation on the intersection of auto racing and science on a cold January Saturday. Just before he took the stage, he said, “Success will look like people realizing that sometimes the cheapest way to go faster is engineering the driver.”
Inside the restored grandeur of the Grand Hall of Michigan Central, downtown Detroit, surrounded by race cars, Ford displays and a crowd of physicians, medical students and curious visitors, Davis stood comfortably between worlds: medicine and motorsports, research and practice, engineering and physiology.
His presentation was part of the Race Days exhibit during the wake of the Formula 1 Red Bull Racing 2026 Car unveilings. The event was held in Detroit because Ford became the engine supplier for the Red Bull F1 team for 2026.
On the surface, it might have appeared to be a niche talk about race cars. It was a story about how medicine, engineering and relentless preparation have quietly reshaped one of the most dangerous sports in the world into one where deaths are no longer considered “normal.”
For decades, motorsport safety focused almost exclusively on the car. Reinforce the chassis. Improve the helmet. Add the halo. Design better barriers. All necessary. All important. But what Davis and the team from Michigan State University's Spartan Motorsport Performance Lab, along with Trifun Dimitrijevski, M.D., chief medical officer of the Detroit Grand Prix, and Chelsea Meixner, R.N., chief nursing director of the Detroit Grand Prix, made clear is that the next frontier of safety is not steel or carbon fiber, it's the human body.
Davis described what happens inside an Indy Car cockpit in a way that made those in the room shift in their seats. No air conditioning. Temperatures reaching 150 degrees in some racing environments. Drivers wearing fireproof Nomex layers, a helmet, gloves and a fire suit. No power steering. Continuous G‑forces similar to what astronauts experience. Repeated braking at the limit, turning at the limit, accelerating at the limit for nearly two hours. Over and over. All race season.
It is, as he put it, “A full body workout under extreme environmental stress while trying not to crash.”
Then Meixner described what happens when a driver enters the medical center after an incident. Drenched in sweat. Elevated blood pressure. Elevated heart rate. Angry, not because they are hurt, but because they cannot finish the race. The vital signs tell the story of the invisible work the body just did.
This is where research meets trackside medicine. At Michigan State University, Davis works under David Ferguson, Ph.D., FACSM, ACSM-CEP, associate professor in the Department of Kinesiology, studying how drivers tolerate heat, G‑forces, dehydration and stress. They simulate cockpit environments using a Lower Body Negative Pressure Chamber Dr. Ferguson received from NASA that was used to train female Astronauts in the 1970s. They train G‑force tolerance. They analyze what happens physiologically before mistakes occur, because mistakes at 180-plus miles per hour have consequences.
Dr. D (Dimitrijevski), as he’s known, added historical context. In the 1970s, Formula One teams were relieved if “only” two drivers died in a season. That was considered “progress.” Today, he said, it’s been more than a decade without a motorsports fatality attributable to a safety failure. That did not happen by accident. It happened because people began asking uncomfortable questions: What is the worst thing that could happen here? How do we prevent it?
Dr. D told a story at turn seven of the Detroit Grand Prix circuit, where the track sits about 40 feet from the Detroit River. Open‑wheel cars can become airborne. Fences can be breached. It is unlikely, but not impossible, for a car to enter the water. So, they station the Detroit Dive and Rescue team and a fire boat there during the entire race weekend. Because “never say never.”
This is what motorsports medicine looks like. Anticipation. Preparation. Refusal to accept “unlikely” as a reason not to plan.
This niche field is becoming formalized. There is now a motorsports medicine fellowship at the Indiana University School of Medicine, recognized by the American College of Physicians and the American Board of Emergency Medicine. Physicians can subspecialize in understanding the physiology, trauma patterns and environmental constraints of motorsports.
The people involved in this work do so because they love it. They do whatever is needed because, as Dr. D said, “If you’re there for the right reason, you’ll love it regardless of what you’re doing.”
It is also a model for interdisciplinary work. Engineers design the cockpit. Physicians and nurses provide care. Researchers study the body and gather data. Rescue teams prepare for the unthinkable. Everyone shares the same goal: the driver goes home.
by Jim Peck
Second-year Michigan State University College of Osteopathic Medicine student Aidan Davis kicked off a presentation on the intersection of auto racing and science on a cold January Saturday. Just before he took the stage, he said, “Success will look like people realizing that sometimes the cheapest way to go faster is engineering the driver.”
Inside the restored grandeur of the Grand Hall of Michigan Central, downtown Detroit, surrounded by race cars, Ford displays and a crowd of physicians, medical students and curious visitors, Davis stood comfortably between worlds: medicine and motorsports, research and practice, engineering and physiology.
His presentation was part of the Race Days exhibit during the wake of the Formula 1 Red Bull Racing 2026 Car unveilings. The event was held in Detroit because Ford became the engine supplier for the Red Bull F1 team for 2026.
On the surface, it might have appeared to be a niche talk about race cars. It was a story about how medicine, engineering and relentless preparation have quietly reshaped one of the most dangerous sports in the world into one where deaths are no longer considered “normal.”
For decades, motorsport safety focused almost exclusively on the car. Reinforce the chassis. Improve the helmet. Add the halo. Design better barriers. All necessary. All important. But what Davis and the team from Michigan State University's Spartan Motorsport Performance Lab, along with Trifun Dimitrijevski, M.D., chief medical officer of the Detroit Grand Prix, and Chelsea Meixner, R.N., chief nursing director of the Detroit Grand Prix, made clear is that the next frontier of safety is not steel or carbon fiber, it's the human body.
Davis described what happens inside an Indy Car cockpit in a way that made those in the room shift in their seats. No air conditioning. Temperatures reaching 150 degrees in some racing environments. Drivers wearing fireproof Nomex layers, a helmet, gloves and a fire suit. No power steering. Continuous G‑forces similar to what astronauts experience. Repeated braking at the limit, turning at the limit, accelerating at the limit for nearly two hours. Over and over. All race season.
It is, as he put it, “A full body workout under extreme environmental stress while trying not to crash.”
Then Meixner described what happens when a driver enters the medical center after an incident. Drenched in sweat. Elevated blood pressure. Elevated heart rate. Angry, not because they are hurt, but because they cannot finish the race. The vital signs tell the story of the invisible work the body just did.
This is where research meets trackside medicine. At Michigan State University, Davis works under David Ferguson, Ph.D., FACSM, ACSM-CEP, associate professor in the Department of Kinesiology, studying how drivers tolerate heat, G‑forces, dehydration and stress. They simulate cockpit environments using a Lower Body Negative Pressure Chamber Dr. Ferguson received from NASA that was used to train female Astronauts in the 1970s. They train G‑force tolerance. They analyze what happens physiologically before mistakes occur, because mistakes at 180-plus miles per hour have consequences.
Dr. D (Dimitrijevski), as he’s known, added historical context. In the 1970s, Formula One teams were relieved if “only” two drivers died in a season. That was considered “progress.” Today, he said, it’s been more than a decade without a motorsports fatality attributable to a safety failure. That did not happen by accident. It happened because people began asking uncomfortable questions: What is the worst thing that could happen here? How do we prevent it?
Dr. D told a story at turn seven of the Detroit Grand Prix circuit, where the track sits about 40 feet from the Detroit River. Open‑wheel cars can become airborne. Fences can be breached. It is unlikely, but not impossible, for a car to enter the water. So, they station the Detroit Dive and Rescue team and a fire boat there during the entire race weekend. Because “never say never.”
This is what motorsports medicine looks like. Anticipation. Preparation. Refusal to accept “unlikely” as a reason not to plan.
This niche field is becoming formalized. There is now a motorsports medicine fellowship at the Indiana University School of Medicine, recognized by the American College of Physicians and the American Board of Emergency Medicine. Physicians can subspecialize in understanding the physiology, trauma patterns and environmental constraints of motorsports.
The people involved in this work do so because they love it. They do whatever is needed because, as Dr. D said, “If you’re there for the right reason, you’ll love it regardless of what you’re doing.”
It is also a model for interdisciplinary work. Engineers design the cockpit. Physicians and nurses provide care. Researchers study the body and gather data. Rescue teams prepare for the unthinkable. Everyone shares the same goal: the driver goes home.
by Jim Peck